
Guest post by Trisha Zhou
In our appearance-obsessed society, we seem to forget that most images we see are an illusion; a thin person can absolutely have coronary heart disease and high cholesterol, and an overweight person, too, can have a restrictive eating disorder. The rampant plastering of the perfect image all over the media extends to the portrayal of what a perfectly sick individual should or shouldn’t look like, and such misrepresentation negatively impacts both those struggling with an eating disorder and the mindset of those around them.
Image credit: New York Times
Nearly all who struggle with an eating disorder have a combination of a deep resentment of the size of their bodies and extreme guilt around their eating habits, whatever they may be they’re a set of thought and behavioral patterns that can occur at any size. However, what we see in the media convinces us that there is only one presentation for an eating disorder emaciated teenage girl who is excessively picky around food and spends hours of her day bathing in vanity, taking romanticized photos of her thigh gap and hip bones protruding from skin-tight jeans. Statistics shows us that in reality:
- 1 in 4 anorexia and bulimia sufferers are men[1]
- Binge eating disorder affects 2.8% of Americans in their lifetime. More often than not, it results in someone being of a normal weight or overweight and is three times more common than anorexia and bulimia combined, as well as being more common than breast cancer and HIV[2]
- 13% of women over the age of 50 have symptoms of an eating disorder[3]
Image credit: Hudson Therapy Group
A psychological disorder, by definition, is a set of thought patterns and resulting behaviors that negatively impact one’s quality of life and ability to function normalizing it isn’t always accompanied by a physically observable presentation. However, because of this one-size-fits-all image that we associate with eating disorders, as well our overall attitude that we can judge someone’s health situation by looking at them, most people in the general public might think someone can only suffer if they fit that image. If someone is overweight, they must be eating burgers on their couch all day, right? They can’t possibly be throwing up their dinners in their bathroom every night. This lack of awareness of how an ED can present itself makes it more difficult to notice if someone is seriously struggling. When they reach out to a family member or friend for help, misinformed beliefs make it unlikely for that person to receive the support and encouragement they need.
On the flip side, those battling with an eating disorder can also see the same stereotypical image in the media and believe that they don’t deserve help until they are dangerously underweight. EDs are classified as egodystonic, meaning that those struggling with it most likely don’t realize the severity of the issue or that they even have a problem. The belief that EDs can only look a certain way further reinforces their belief that they don’t need help.

Image credit: Acacia Dreams
When someone finally musters up the courage to get an appointment with a doctor, they’re often dismissed if they aren’t underweight. In fact, many overweight BED or bulimia patients are told by physicians that they need to prioritize weight loss, despite the fact that their EDs feed off of shame about their body and guilt around eating food, driving them further into their self-destructive behaviors. Anorexia sufferers of a normal or higher weight aren’t provided with the treatment they desperately need, although we know that any type of disordered eating behavior has lasting physical and psychologist impacts, such as hair loss, amenorrhea, electrolyte imbalance, depression, and isolation from family and friends. Inpatient eating disorder treatment centers usually have a long waiting list and don’t accept patients unless they are under an extremely low BMI threshold. And those who, by society’s standards, are too old to be dealing with a teenage problem feel that they shouldn’t talk about their struggles due to the stigma.
The later someone receives the help they need, the more dire the consequences. While we know that 1 in 4 anorexia and bulimia sufferers are men, they have a higher mortality rate due to delayed seeking of treatment as a result of stigma; anorexia sufferers between the ages of 15 and 24 have 10 times the mortality rate compared to peers of the same age and while anorexia has the highest mortality rate of any psychological disorder, one in five anorexia deaths is by suicide.[4]
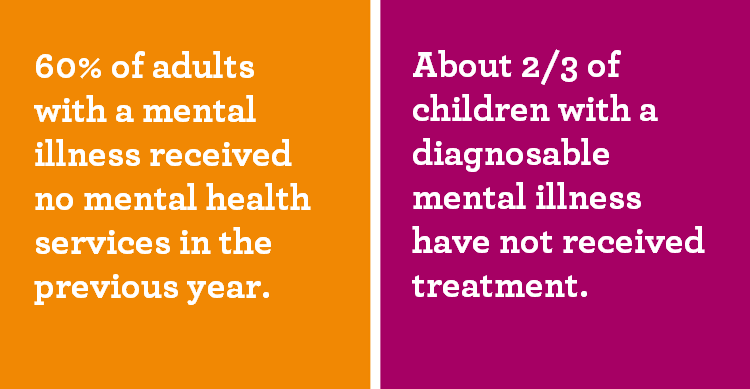
Image credit: Legacy Community Health
Eating disorders are ugly. They aren’t a dieting phase in a young woman’s rite of passage; they are isolation from people you love and apathy for all the hobbies you cared about. They don’t always look like someone eating carrots to drop a few pounds for a photoshoot or big event; instead, they are screaming fights at the dinner table and crying yourself to sleep every night. Most of all, they aren’t a choice, or a nightmare that you can magically and abruptly snap out of.
So, what can we do?
- If you have a friend or family member who is struggling with an eating disorder, read up about what is and isn’t true of EDs, which can help you better support them. Understand that although they are not yours to fix or solve, they can benefit from knowing that they have your support. Encourage them to seek professional help from a psychologist, psychiatrist and/or an eating disorder specialist dietitian, even if it might take a few tries to find a good fit.
- If you are struggling yourself, I’m thinking of you. Reach out to someone you trust and tell them about what’s going on. Please seek professional help if you are able to and haven’t already. Remember to take things a day at a time, or a week, an hour of a time if you need to.
- If you have recovered from an eating disorder, congratulations! It is an arduous journey that requires such patience and strength. You must be so proud of yourself! Keep up the good work.
- If you don’t know of anyone who’s struggling around you, keep reading about it and help break the stigma. As always, check in on your friends and family; you never know what someone’s going through and if they might need some extra support. Let people around you know that they can count you for a listening ear.

Image credit: NAMI
References
[1] Keski-Rahkonen A, Hoek HW, Susser ES, Linna MS, Sihvola E, Raevuori , and Rissanen A. (2007). Epidemiology and course of anorexia nervosa in the community. American Journal of Psychiatry, 164(8):1259-65. doi: 10.1176/appi. ajp.2007.06081388.
[2] Hudson JI, Hiripi E, Pope HG Jr, and Kessler RC. (2007). The prevalence and correlates of eating disorders in the National Comorbidity Survey Replication. Biological Psychiatry, 61(3):348-58. doi:10.1016/j.biopsych.2006.03.040.
[3] Source: Gagne, D. A., Von Holle, A., Brownley, K. A., Runfola, C. D., Hofmeier, S., Branch, K. E., & Bulik, C. M. (2012). Eating disorder symptoms and weight and shape concerns in a large web based convenience sample of women ages 50 and above: Results of the gender and body image (GABI) study. International Journal of Eating Disorders, 45(7), 832-844.[4] Source: Arcelus, J., Mitchell, A. J., Wales, J., & Nielsen, S. (2011). Mortality rates in patients with anorexia nervosa and other eating disorders: a meta-analysis of 36 studies. Archives of General Psychiatry, 68(7), 724-731.
Trisha Zhou is a New-York based RD2Be and volunteer at DishWithDina. She is currently pursuing a degree in piano performance. Learn more about Trisha’s personal story here.


0 Comments